Two Types Of Kidney Dialysis:
|
CEU Test #93 "Chronic Kidney Disease". by Sylvie Mulvaney. (Posted 3/8/2017)
When Kidneys Fail Dialysis filters toxins from the blood. During treatment, a special fluid mixture of pure water and chemicals pulls waste, salt and extra water from the blood, leaving behind essential substances such as potassium and other electrolytes. Not surprisingly, many people report feeling much better after dialysis treatments. There are two types of dialysis treatments for people with ESRD: hemodialysis and peritoneal dialysis. Hemodialysis can be performed in a dialysis center or in a patient’s home with assistance from a trained care partner. During treatment, the patient is attached via needle stick to a special-access area of the body (dis-cussed in more detail several para-graphs down) to a dialysis machine about the size of a dishwasher. (See Photo 1)
The patient’s blood passes through a large canister called a dia-lyzer – often called an artificial kidney – which contains thousands of small fibers. Dialysate, the cleansing solution, contains chemicals that make it act like a sponge. It is pumped around the fibers, allowing waste and extra fluids to pass from the blood into the solution, and out of the body. The filtered blood is then returned to the body.
There are two permanent types of hemodialysis access.
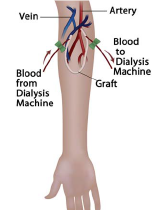
An arteriovenous (AV) fistula is the most dependable type of access. It is made by directly connecting an artery to a vein beneath the skin, usually in the upper arm or forearm. (See Photo 2) As blood flows to the vein from the newly connected artery, the vein grows bigger and stronger, and can provide good, dependable blood flow for many years of hemodialysis. Fistulas tend to last longer than grafts, and are less likely to incur complica-tions, such as infections or blood clots. For this reason, fistulas widely are considered “the gold standard” access choice. Fistulas need several months to heal, or mature, before they can be used for hemodialysis.
Most hemodialysis patients require treatment three days a week, usually Monday-Wednesday-Friday or Tues-day-Thursday-Saturday, for as much as four hours a day. During treat-ments, patients can sleep, read, write, talk or watch TV. Of course, there are times when emergent dialysis is needed on a Sunday or during the night. Some patients also choose noc-turnal hemodialysis, which can take place at a center, overnight, while they sleep. The nocturnal dialysis process takes longer and some patients report difficulty sleeping during the procedure, while others prefer it because it provides them more free time during daylight hours to live their lives.
An AV graft is made by inserting a small, soft tube between an artery and a vein, also usually in the upper arm or forearm, but sometimes in the thigh near the groin. (See photo 4) Grafts are a good choice for patients with small veins, and sometimes can be used as soon as one week after placement. Grafts might not last as long as fistulas, however, and are more likely to become infected or narrow and cause blood clots.
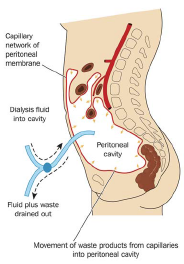
For patients requiring hemodialysis before their fistula or graft is ready for use, a short-term central venous catheter (CVC) might be placed in the neck or chest. A CVC often is a double-lumen access placed in the right anterior chest wall. Peritoneal dialysis (PD) is a needle-free treatment patients can perform themselves at home or at work. Via a surgically placed catheter in the abdomen, PD uses the lining of the patient’s abdomen to filter blood. This lining, called the peritoneal membrane, acts as the artificial kidney. There are three types of PD available, which need not be dis-cussed here. (Continued) |
Generally, PD works like this: a dial-ysis solution of certain minerals and dextrose, or sugar, water travels through the catheter into the patient’s abdomen. The dextrose pulls waste, chemicals and extra water from the peritoneal membrane’s tiny blood vessels into the dialysis solution. After several hours of “dwell time,” the solution is drained from the abdomen through the same catheter, taking the wastes from the blood with it. (see photo 5) The abdomen is again filled with fresh dialysis solution, and the cycle is repeated. The draining-refilling process is called an exchange.
The most common problem with PD is peritonitis, a serious abdominal infection, which can occur if the catheter insertion site becomes infected or if contamination occurs during the draining-refilling proce-dure. Some people report reserving one room in their home as their PD sterile room, restricting access to family members, visitors and pets in an effort to maintain as clean an environment as possible. Depending on their overall health, patients can be on dialysis for many years before a suitable donated organ is found, or until their health declines and they ultimately die. We Encourage you to read the entire article on Vitals, or other archived CEU articles from the Gold Cross Magazine


To subscribe to Gold Cross Magazine, please call Leonard Publications at 973-895-6000 or fill in the form below.
Annual price per subscriber is $16.00 Special Group Pricing There is a reduced price of $15.00 per subscription to any squad that either:
|